
Recently, I’ve been following the work of the Lincoln-Lancaster County Board of Health to learn more about the Board’s duties and how it operates.
Reconciling small differences
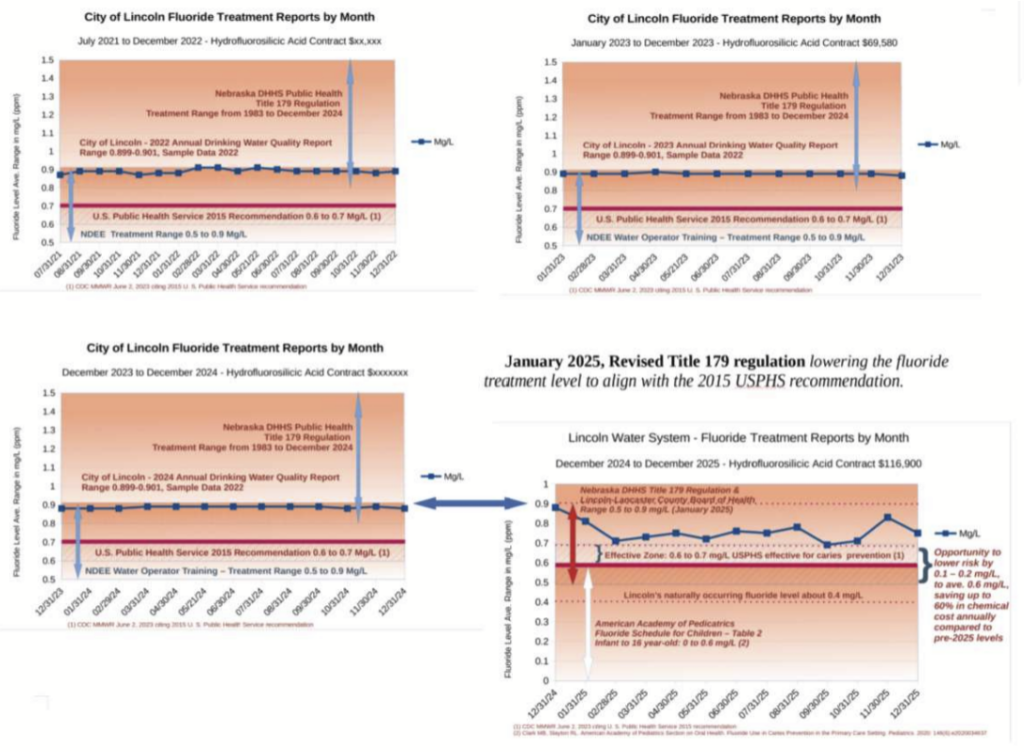
As background, I began my search for understanding about how public health in Nebraska operates by checking out drinking water fluoridation in Lincoln (a recent post is here). After little progress in reconciling the differences I found, I asked for help from Governor Pillen and DHHS Director Corsi. This petition may have, in part, prompted NE DHHS to revise its 1983 treatment level regulation to align with the 2015 recommendations of the USPHS and the CDC. In January 2025, the City of Lincoln responded to this revision by effectively lowering the treatment level by about 1 point.
In an effort to lower the treatment level by another point, to further reduce risk and cost, I provided open comment at the Board’s February meeting by highlighting upper daily intake risks and requesting their recommendation (my comment with attachmented treatment reports, dosing information and daily exposure). The Board’s February minutes summarize my comments.
Highlighting larger differences
During the February meeting, Board members discussed their strong opposition to the legislative bill, LB203, requiring approval from the elected city and county officials serving on the Board before a health director can issue a community-wide directed health measure. In its comments, submitted to the HHS committee hearing for LB203, the Board made the following points:
- The Health Department’s quick action in responding to infectious disease threats, including COVID-19, measles, and mpox (formerly monkeypox), controlled the spread of disease.
- Swift action is critical to ensuring health and safety.
- The Director uses many data sources and consults with many local and national experts in decision-making to identify actions for specific infectious diseases.
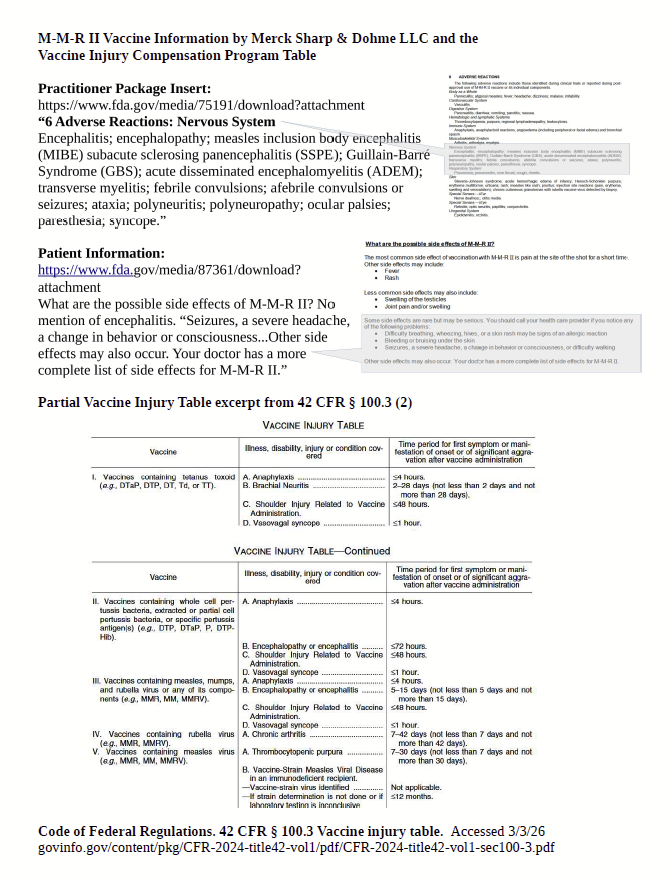
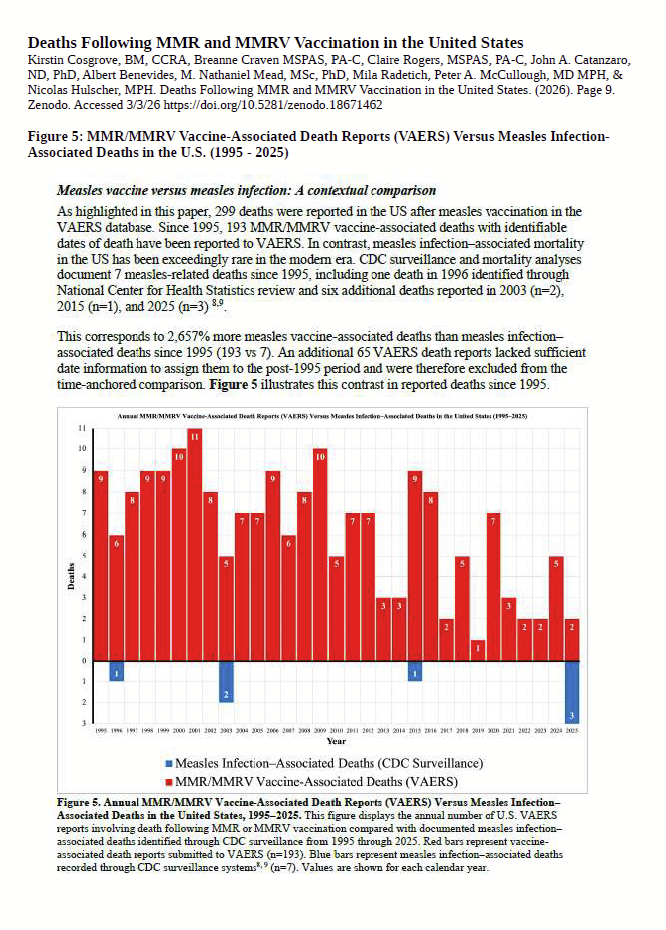
I addressed these points, through comments, at the Board’s March meeting, attempting to focus on shared core values, trust and faith, and by asking several questions about what consent looks like, between patient-doctor and in governance, and by asking, “how do we build the trust that the Board and others expect, in a culture that disregards well-qualified experts who demand examination of vaccine safety (see my comments, questions, and attachments 1, 2, 3, and 4)?”
In following the work of the Board, I seek: increased awareness of different perspectives and interpretations of scientific evidence; transparent and inclusive community input on policies, procedures and operations; and, to build the capacity for individuals, with diversity of thought and experience, willing to serve, and to be accepted to serve, on the Board.
Comments are welcomed. Send to admin@lincolnsopensource.com