“Community water fluoridation is the process of adjusting the fluoride content of fluoride-deficient water to the recommended level for optimal dental health, which is currently recommended at 0.7 parts fluoride per million parts water.” emphasis added
American Dental Association, Topic Update 7/14/2023, archive copy
Contents
- Summary Points
- City of Lincoln’s & State Public Records Requests
- Lancaster County Response to Request for Information
- State Response to Request for Information
- References & Links
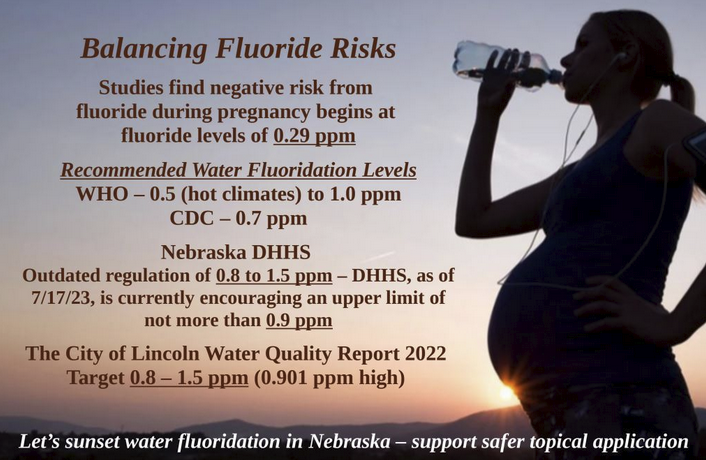
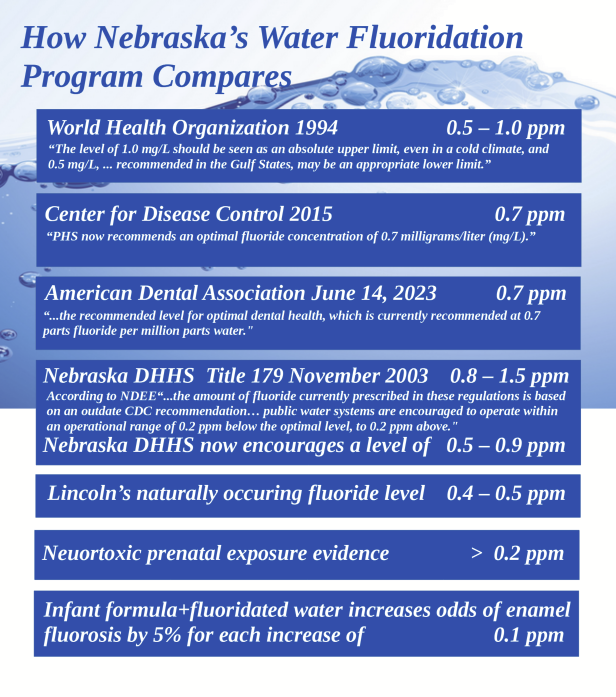
According to the Nebraska Department of Environment & Energy, July 2023, “The amount of fluoride currently prescribed in [the water supply regulations] is based on an outdated CDC recommendation regarding optimum fluoride levels (0.9 – 1.0 ppm). In 2015 CDC updated their recommended optimum level to 0.7 ppm.”
The American Dental Association, Topic Update 7/14/23 says, “Community water fluoridation is the process of adjusting the fluoride content of fluoride-deficient water to the recommended level for optimal dental health, which is currently recommended at 0.7 parts fluoride per million parts water.” and recommends unfluoridated water for infant formula through at least age 12 months.
Calculated fluoride values for the City of Lincoln in July and August 2023 ranged from 0.88 – 0.90 mg/L, exceeding the recommended level of both the CDC and the American Dental Association.
Join the conversation by contacting your dentist, the City Council, the Lancaster County Board of Health & County Commissioners, the Nebraska Department of Health & Human Services – Public Health, and your State Senator.
Let’s sunset water fluoridation in Nebraska – support safer topical application
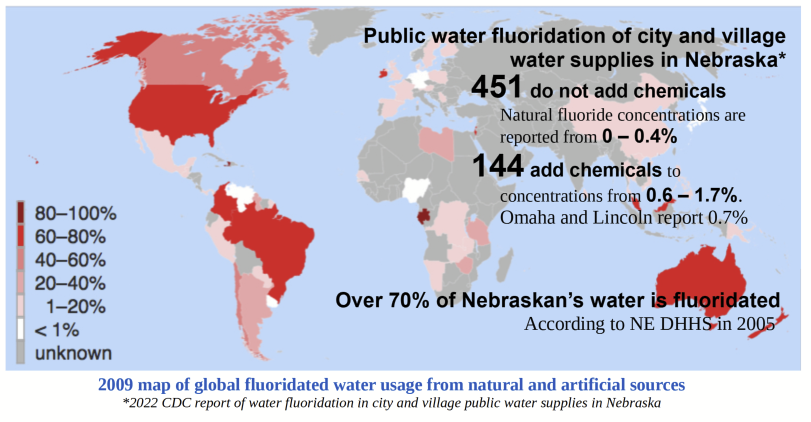
Lincoln’s naturally occurring water fluoride level ranges from 0.4 to 0.5 ppm.
- Fluoride & IQ: The U.S. DHHS National Toxicology Program Review and other studies indicate a link between fluoride exposure and cognitive health
- Infant Formula: The American Dental Association supports breast-feeding and recommends unfluoridated water for infant formula to reduce risk of tooth mottling, called fluorosis
- Essential to consider all fluoride sources: WHO Guidelines for Drinking-water Quality, consider all fluoride exposure from beverages, food, and environment
- Unsettled questions about fluoride exposure safety: National Academies of Science – National Research Council 2006 report of Fluoride in Drinking Water
A Benchmark Dose Analysis for Maternal Pregnancy Urine-Fluoride and IQ in Children, 2020:
A benchmark concentration for maternal urinary fluoride of 0.29 ppm was associated with a 1-point decrease in IQ scores of preschool-aged boys and girls
A 5-minute video showing how a small drop in IQ effects the overall population
Little Things Matter, (accessed 13 November 2024, 25 July 2023 – link removed)
Dietary fluoride intake during pregnancy and neurodevelopment in toddlers: A prospective study in the progress cohort
A 0.5 mg/day increase in overall dietary fluoride intake was associated with a 3.46-point lower cognitive outcome in boys
U.S. Department of Health & Human Services National Toxicology Program
Monograph on the State of the Science Concerning Fluoride Exposure and Neurodevelopmental and Cognitive Health Effects: A Systematic Review September 2022
“1.5 ppm is consistently associated with lower IQ in children. More studies are needed to fully understand the potential for lower fluoride exposure to affect children’s IQ.”
Journal of the American Dental Association, January 2011
“… the greater the amount of fluoride intake during tooth development in any person, the greater the prevalence of fluorosis development… Practitioners should be aware that children are exposed to multiple sources of fluoride during the tooth development period. Reducing fluoride intake from reconstituted infant formula alone will not eliminate the risk of fluorosis development. It also is important that clinicians provide advice to parents regarding the proper use of fluoridated toothpastes along with the informed prescription of fluoride supplements. The panel acknowledges and encourages clinicians to follow the American Academy of Pediatrics’ guidelines for infant nutrition, which advocate exclusive breastfeeding to age 6 months and continued through at least age 12 months unless specifically contraindicated. Human breast milk has been shown to have consistently low levels of fluoride.”
The City of Lincoln Water Quality Report 2022
NE DHHS Title 179 Public Water SystemRules & Regulations Governing Fluoridation of Water Supplies:(pg 309)
Appendix A to Title 179 NAC 14– Fluoride 4 ppm MCLG,
Major Sources in drinking water: Erosion of natural deposits; Water additive that promotes strong teeth; Discharge from fertilizer and aluminum factories.
Health effects language: Some people who drink water containing fluoride in excess of the MCL over many years could get bone disease, including pain and tenderness of the bones. Fluoride in drinking water at half the MCL or more may cause mottling of children’s teeth, usually in children less than nine years old. Mottling, also known as dental fluorosis, may include brown staining and/or pitting of the teeth, and occurs only in developing teeth before they erupt from the gums.
The Fluoride Debate: The Pros and Cons of Fluoridation
Conclusion: Since the fluoride benefit is mainly topical, perhaps it is better to deliver fluoride directly to the tooth instead of ingesting it.
Fluoride Toxicity (7/28/2023)
“For optimal dental health, the World Health Organization recommends a level of fluoride from 0.5 to 1.0 mg/L (milligrams per liter), depending on climate.[6] Fluorosis becomes possible above this recommended dosage. As of 2015, the United States Health and Human Services Department recommends a maximum of 0.7 milligrams of fluoride per liter of water – updating and replacing the previous recommended range of 0.7 to 1.2 milligrams issued in 1962. The new recommended level is intended to reduce the occurrence of dental fluorosis while maintaining water fluoridation.[7]”
Citation [6] page decommissioned Archived (PDF) from the original on 2015-02-17. Retrieved 2013-09-01.WHO Expert Committee on Oral Health Status and Fluoride Use (1994). Fluorides and oral health (PDF). WHO technical report series 846. Geneva: World Health Organization. ISBN92-4-120846-5.
Archived 1994 World Health Organization, Fluoride and Oral Health
Relating to the fluoride dose as dependent on the amount of water ingested, “The level of 1.0 mg/L should be seen as an absolute upper limit, even in a cold climate, and 0.5 mg/L, now used in Hong Kong and recommended in the Gulf States, may be an appropriate lower limit.
Wold Health Organization Guidelines for Drinking-water Quality 2017
Referencing the need to filter very high naturally occurring fluoride levels, “There is no evidence to suggest that the guideline value of 1.5 mg/l set in 1984 and reaffirmed in 1993 needs to be revised. Concentrations above this value carry an increasing risk of dental fluorosis, and much higher concentrations lead to skeletal fluorosis. The value is higher than that recommended for artificial fluoridation of water supplies, which is usually 0.5–1.0 mg/l.
In setting national standards or local guidelines for fluoride or in evaluating the possible health consequences of exposure to fluoride, it is essential to consider the average daily intake of water by the population of interest and the intake of fluoride from other sources (e.g. from food and air). Where the intakes are likely to approach, or be greater than, 6 mg/day, it would be appropriate to consider setting a standard or local guideline at a concentration lower than 1.5 mg/l.”
Profits in public and residential water treatment

Summary Points
- Nebraska’s required fluoride level is too high: the specified fluoridation range of 0.8 – 1.5 ppm is above both CDC and WHO recommendations, 0.7 ppm and 0.5 – 1.0 ppm respectively. (4)(5)(6)
- NE DHHS regulations give communities 12 months to notify the public if levels exceed 2.0 ppm (6)
- The position that ingesting fluoride helps less fortunate children and adults with problems of tooth decay was proven wrong: Dr. Weston A. Price, Chairman of The Research Commission of The American Dental Association, documented in his 1939 book Nutrition and Physical Degeneration that mineral and vitamin levels determine incidence of dental caries, not fluorine content of the water supply. Dr. Price wrote that fluorine content cannot compensate for diets “terribly deficient in many minerals and vitamins.” (See Research Document Pg 6)
- Fluoridated drinking water does not save Medicaid spending: as proven by the research of Dr. Weston Price, dental caries, in addition to overall disease, are a symptom of a nutrient-deficient diet, not a single chemical deficiency. Fluoride’s primary effect is topical, not systemic and there is no difference in tooth decay between fluoridated and non-fluoridated countries. (See Research Document Pg 5-6)
- A safe exposure level for fluoride in pregnancy has not been established: study recommends revising water fluoridation regulation level of 0.7 mg/L based on strong evidence of prenatal neurotoxicity at levels of 0.2 mg/L or slightly below. (1)
- Fluoride level of 1.5 ppm is consistently associated with lower IQ in children, more studies needed for affects of lower exposures: as reported by the U.S. DHHS National Toxicology Program’s report on the toxicity of fluoride. Three public water systems in Nebraska report levels above 1.5 ppm. (2)(3)
- Cost to treat a questionable need: As noted in the 2022 Omaha MUD Water Quality Report, the Missouri and Platte Rivers have naturally-occurring fluoride in the range of 0.3 to 0.5 parts per million (ppm). What is the cost to increase the naturally-occurring fluoride level the 0.2 – 0.4 ppm up to the CDC recommended level of 0.7 ppm? (7)
- Increased susceptibility to harms: Similar to harms from non-ionizing magnetic and radio frequency fields, body metabolism and recovery strength varies based on a variety of factors like age, pregnancy, nutrient deficiencies, disease state, and overall toxic load from foods, beverages, and industrial pollution. What may be considered a less harmful dose of fluoride for one individual may be toxic for another. “Evidence reviewed about 15 years ago suggested that sufficient information was available to warrant further consideration of the possible adverse effects of fluoride exposure with an emphasis on vulnerable populations.” National Research Council 2006 (See Research Document Pg 8)
- Historical view of public policy, consensus-based, profit-driven public relations campaigns based on a politically motivated working hypothesis have been very successful in shaping public policy. Contagion theory has had similar effects on how the public perceives health care and food. Here are three examples highlighting the healing world of personal accountability versus a world of fear. (See Research Document Pg 9)
- Antoine Béchamp vs Louis Pasteur – terrain versus germ theory
- Del Bigtree vs Neil deGrasse Tyson – evidence and logic versus consensus-based science
- Steve Kirsh vs Mark Bailey et al. – working hypothesis in the debate on virus as a contagion
A tale of two dentists in the 1930’s and 1940’s, nutrient-dense food or medicine?
Dr. Weston A. Price traveled the world to study and write about the healthy teeth of people living on traditional diets. Then, as now, many dentists were convinced that modern food processing, particularly of flour and sugar, were largely to blame for increased incidents of cavities in the early 1900’s.


Dr. Trendley Dean, WWI Army veteran and dentist, became a key figure at the National Institutes of Health and, with support of the American Dental Association, had a key role in transforming fluoride’s medical image from tooth disfigurer to a cavity preventative. He, and others, secured his claim by writing articles about the necessity of medicating public water supplies with fluoridating chemicals.
References & Links
- A Benchmark Dose Analysis for Maternal Pregnancy Urine-Fluoride and IQ in Children, 2020: “As a safe exposure level for fluoride in pregnancy has not been established, we used data from two prospective studies for benchmark dose modeling…. Evidence reviewed about 15 years ago suggested that sufficient information was available to warrant further consideration of the possible adverse effects of fluoride exposure with an emphasis on vulnerable populations (National Research Council 2006). Only now has thorough prospective epidemiology evidence become available on populations exposed to fluoridated water (about 0.7 mg/L) or comparable exposure from fluoridated salt. The prospective studies offer strong evidence of prenatal neurotoxicity and should inspire a revision of water-fluoride regulations based on the benchmark results, especially for pregnant women and young children… These findings, using a linear concentration dependence, suggest an overall [benchmark concentration level] BMCL for fluoride concentrations in urine of approximately 0.2 mg/L or slightly below that level.” https://pubmed.ncbi.nlm.nih.gov/33173917/ and https://fluoridealert.org/studytracker/39766/
- U.S. Department of Health & Human Services National Toxicology Program 2023 (See Research Document Pg 2):
- “1.5 ppm is consistently associated with lower IQ in children. More studies are needed to fully understand the potential for lower fluoride exposure to affect children’s IQ.” https://ntp.niehs.nih.gov/whatwestudy/assessments/noncancer/ongoing/fluoride https://ntp.niehs.nih.gov/ntp/about_ntp/bsc/2023/fluoride/documents_provided_bsc_wg_031523.pdf
- Nebraska cities or villages that fluoridate to concentrations above 1.5 ppm ;
- As reported to CDC in 2022 – Verdel 1.7, Winnebago Kelley Project and Winnebago Village 1.6
- World Health Organization, Fluoride and Oral Health, 1994(See Research Document Pg 6); “Relating to the fluoride dose as dependent on the amount of water ingested, “The level of 1.0 mg/L should be seen as an absolute upper limit, even in a cold climate, and 0.5 mg/L, now used in Hong Kong and recommended in the Gulf States, may be an appropriate lower limit.” https://en.m.wikipedia.org/wiki/Fluoride_toxicity#cite_ref-WHO-TRS-846_6-0 Archive – https://web.archive.org/web/20120123194052/http://whqlibdoc.who.int/trs/WHO_TRS_846.pdf
- CDC U.S. Public Health Service recommendation for community water fluoridation, 2015 (See Research Document Pg 7);
“PHS now recommends an optimal fluoride concentration of 0.7 milligrams/liter (mg/L).”
- State of Nebraska DHHS Title 179 Public Water System Rules & Regulations Governing Fluoridation of Water Supplies, 0.8 – 1.5 ppm (See Research Document Pg 4);
- Ch 1 003.01 – “the fluoride ion content of the water available to users, as prescribed by the State Department of Health, shall be in the range of 0.8 to 1.5 parts per million, the recommended optimal level being 1.0 to 1.3 parts per million.”
- Ch 2-002.04A “Community water systems experiencing fluoride levels above 2.0 milligrams per liter must notify the public as required”
- Ch 4 -010.01 – “Public notice must be provided as soon as practical but no later than 12 months from the day the water system learns of the exceedance.” https://dhhs.ne.gov/Documents/Title-179-Complete.pdf
- Fluoridation of select Nebraska cities, as reported to CDC for 2022, mg/L = ppm; https://nccd.cdc.gov/DOH_MWF/Reports/FlStatus_Rpt.aspx
- 0.7 ppm Douglas County MUD, CDC 0.70 mg/L, Omaha MUD 2022 report 0.571 – 0.806 ppm
- 0.8 – 1.5 ppm Lincoln, CDC 0.70 mg/L, City of Lincoln 2022 reports 0.899 – 0.901 ppm
- Kearney, CDC 0.70 mg/L
- Blair, yes, CDC reports 0.70 mg/L, Blair Annual Quality report event viewer requires password. https://www.blairnebraska.org/2347/Annual-Water-Quality-Report
- 0.7 ppm Douglas County MUD, CDC 0.70 mg/L, Omaha MUD 2022 report 0.571 – 0.806 ppm
- Chemicals used;
- Lincoln, hydrofluorosilicic acid sold by Hawkins, Inc. annual purchase 350,000 pounds/year, $69,580
- Fluoride Mandate: Nebraska State Statute 71-3305 mandates for cities or villages over one thousand or more inhabitants (See Research Document Pg 3);
- Cities or villages (with some exceptions) shall add fluoride as “provided in the rules and regulations of the Department of Health and Human Services unless such water supply has sufficient amounts of naturally occurring fluoride as provided in such rules and regulations” https://nebraskalegislature.gov/laws/statutes.php?statute=71-3305
- Larger Nebraska communities that do not fluoridate;
- Grand Island, Hastings, North Platte, Norfolk, Scottsbluff, Beatrice, Lexington, York – Passed in 2008 after mandate Plattsmouth, Wisner, 2010 Saunders County, Wahoo (after approving fluoridation in 2008) https://nccd.cdc.gov/DOH_MWF/Reports/FlStatus_Rpt.aspx
- NE DHHS Oral Health Surveillance System Report, 2011 – 2020Nebraska communities with high levels of naturally occurring fluoride; none, all non-fluoridated communities have concentrations at 0.50 or below. https://nccd.cdc.gov/DOH_MWF/Reports/FlStatus_Rpt.aspx
- Nebraska industries emitting fluoride pollution;
- none, all non-fluoridated communities have concentrations at 0.50 or below. https://nccd.cdc.gov/DOH_MWF/Reports/FlStatus_Rpt.aspx
- Nebraska industries emitting fluoride pollution;
- Public utilities, corn and mineral production https://fluoridealert.org/researchers/overview-tri/ (see new link to EPA’s TRI Program site https://www.epa.gov/toxics-release-inventory-tri-program)
Additional Links
- Hujoel PP, Zina LG, Moimaz SA, Cunha-Cruz J. Infant formula and enamel fluorosis: a systematic review. J Am Dent Assoc. 2009 Jul;140(7):841-54. doi: 10.14219/jada.archive.2009.0278. PMID: 19571048.
- Release of NTP’s Fluoride Toxicity Report, March 15, 2023
- A judge’s ruling forced the Department of Health and Human Services to release the National Toxicology Program’s report on the toxicity of fluoride. Attorneys’ with the Fluoride Action Network negotiated this release of information.
- Scroll down to find March 15, 2023 post
“This review finds, with moderate confidence, that higher fluoride exposure (e.g., represented by populations whose total fluoride exposure approximates or exceeds the World Health Organization Guidelines for Drinking-water Quality of 1.5 mg/L of fluoride) is consistently associated with lower IQ in children. More studies are needed to fully understand the potential for lower fluoride exposure to affect children’s IQ.” A reviewer’s related comment, regarding limited studies at lower exposures, “as there are few studies that provide evidence of this for exposures in the low range. This is not to say that there is no association at these lower levels, there may very well be an association; just that these results cannot be generalized to lower levels of exposure. This is true with other neurotoxins as well, for example, we know that the associations between lead and IQ scores is even steeper at the lower levels of exposure, but early studies where exposure was high were not able to discern those associations.” Emphasis added.
DRAFT NTP Monograph on the State of the Science Concerning Fluoride Exposure and Neurodevelopmental and Cognitive Health Effects: A Systematic Review, September 2022
Page 13, Released March 15, 2023
Public Records Requests: City of Lincoln and Lancaster County, State DHHS and NDEE
March 2, 2023 request for information on fluoride – after two follow-up emails and a requested opinion from the Mayor 4/11/2023 regarding the 3/2/23 email request, the posting of the city’s 2022 Water Quality Report and the March 15, 2023 release of the DHHS National Toxicology Program’s Monogram on the State of the Science Concerning Fluoride Exposure and Neurodevelopmental and Cognitive Health Effects (NTP report). The email requested the Mayor’s opinion on the NTP report as it relates to fluoridation of the city’s water supply and the potential liability the city may incur from the findings. A hearing was held the same day in the ongoing federal lawsuit against the U.S. Environmental Protection Agency over the use of neurotoxic fluoridation chemicals.
Response by City of Lincoln Transportation and Utilities
April 11, 2023 response from the Assistant Director, Utilities
“Fluoridation of Lincoln’s water has been done since 1970. As we understand, fluoridation started following a vote of the people which is how communities dealt with deciding on this topic many years ago. In 2008, the State of Nebraska passed a law preventing communities with populations over 1,000 to repeal fluoridation. So, that leaves Lincoln being required to continue fluoridating its water and would require an act of the Nebraska Legislature to reverse.
It has been widely accepted that fluoridation prevents tooth decay and is supported by the American Dental Association. The Lincoln Water System must follow State of Nebraska drinking water regulations which currently requires a minimum fluoride level in its water supply.
If Federal regulations should require discontinuing use of fluoride, legislation would be necessary in Nebraska legislature and Lincoln would then follow the new Nebraska law.” End of response.
City of Lincoln, NE, Water Quality Report 2022 – see link to the city contract for Hawkins, Inc. on page 9.
Fluoride: Highest test result – 0.901 ppm, Range or Test Results – 0.899-0.901 ppm, Sample Date – 2022, Highest Level Allowed – 4 ppm, MCL Goal – 4 ppm.
Report Footnote: Fluoride is added in treatment to bring the natural fluoride level of about 0.4 ppm to the State recommended level of 0.8 – 1.5 ppm. LWS continuously monitors the fluoride level in the water.
Lincoln & Lancaster County Health Department
September 20, 2024 – Email sent to Director Pat Lopez to clarify a conversation and request for records, “It was nice to meet you yesterday at the CHE open house and I appreciate talking with you briefly about my fluoride information request.
I have just a few more questions of utmost concern due to studies showing negative impacts from fluoridation level increases in preborn and infants of even 0.1 ppm. The June 2023 CDC MMWR that Donna shared with me
summarizes in the last paragraph with this quote, “CDC continues to emphasize the importance of community water fluoridation at the recommended level of 0.7 mg/L as the cornerstone of dental caries prevention in the United States.” https://www.cdc.gov/mmwr/volumes/72/wr/pdfs/mm7222-H.pdf
I understood you to say that you had an epidemiologist review my request and that they assured you that the current fluoridation level that Donna provided to me is safe. Donna referenced State regulations that I understand are out of date, 0.8 – 1.5 ppm. If this is correct, are there written findings or communication on this determination that you can
provide to me? And, was this a County staff determination or has the State issued written updates? I am looking for a written official fluoridation level, as I have not received further response from Nebraska DHHS.
As I shared with you, I disagree with these findings because I feel I did not receive a complete answer to my question. Based on my research indicating that both the CDC and the American Dental Association recommend a
maximum fluoride level of 0.7 ppm, and the ADA recommends non-fluoridated water for infants, I would still like to see exactly where the County’s recommendation is coming from and the specific citation in the document Donna referenced above, if this is the source of the County’s recommendation.” End of email. No written response has been received from Director Lopez.
NDEE, DHHS and City of Lincoln Record Requests
June 30, 2023 – Records request to NDEE for state fluoride regulations and fluoride operations records sheets for Lincoln. July 14, 2023 2nd request follow-up
July 14, 2023 Response from NDEE DW Field Services, “The education and oversight of fluoridating public water systems in Nebraska, and the individuals responsible for operating them, is a cooperative effort between staff within the Drinking Water & Groundwater Division here at NDEE,
and the Nebraska Dept. of Health and Human Services, Office of Oral Health.
“Regulations related to public water supplies in Nebraska are currently found in Title 179. While some more general requirements such as operation & maintenance, system design, and reporting/recordkeeping, can be found in other chapters of Title 179, regulations specifically related to the fluoridation of public water supplies are found in Title 179
Chapter 1. I have attached a copy of this chapter for your reference. Requirements specific to the operation of a water system’s fluoridation program are found in Section 003 of that chapter, including the amount of fluoride in finished water, record keeping, and reporting requirements. The amount of fluoride currently prescribed in these regulations is based on an outdated CDC recommendation regarding optimum fluoride levels (0.9 – 1.0 ppm). In 2015 CDC updated their recommended optimum level to 0.7 ppm. While Chapter 1 does not reflect that change at this time, public water systems are encouraged to operate their fluoridation programs according to the updated recommendation, working within an operational range of 0.2 ppm below the optimal level, to 0.2 ppm above. [emphasis added]
“Attached are the monthly fluoridation reports submitted by Lincoln Water System for the past two years. These reports provide a daily calculated concentration of fluoride in the water produced. These calculations are based on the volume of water produced, the amount of chemical used, and the natural fluoride content of the source water. Lincoln Water System has two water plants. Each month they submit a report for each plant. If that plant was not in use during part, or all, of a given month, the report will be blank for that period. I have also attached a summary of the results from finished water fluoride samples collected from Lincoln Water system over that same two-year period.” End of email response.
July 17, 2023 – Follow-up request for information to NDEE and City of Lincoln, request 1) process for revising the relevant portions of Title 179 and for developing the recommended dosing level required, a copy of notification sent to public water systems to revise Title 179 required operational fluoridation level, 2) question: how do fluoride sample results relate to range documented in the 2022 Lincoln Water Quality Report, 3) clarification from the City regarding comment that reference in MMWR Weekly 6/2/2023 refers to 0.7 mg/L is a minimum fluoride level. Fluoride reports provided by Lincoln on 9/12/23 and response from Assistant Director, Utilities on MMWR level, “the range recommended was between 0.7 mg/L to a maximum of 2.0 mg/L. You are correct that less than 0.6 mg/L is ineffective in preventing dental caries.”
October 5 & 18, 2023 – Follow-up to July 17 request #1 and #2 with clarification, 1) disparity in fluoridation level – Lincoln fluoride levels above CDC recommendation, 2) request for records used by the Health Director to determine safe fluoridation level and to inform the Board and the public, 3) documentation of changed fluoride level communication between City-County and State, documents to demonstrate understanding, guidance and implementation of the fluoridation program.
October 25, 2023 – Response from NDEE, program staff is working on initial identification of communications responsive to request and suggestion/offer to modify or prioritize any items in the request
October 27, 2023 – Modified records request for common practice, clear and current regulations, directions/procedures, and understanding between City of Lincoln and the State regarding fluoridation due to apparent disparity in treatment level.
November 1, 2023 – NDEE response requesting clarification seeking multiple documents or single document. Provided link to fluoride treatment reports (see portal link below)
November 3, 2023 – Request for records clarified to single, most current documents, add request #4, staff review or any current opinions or findings on fluoridation.
November 13, 2023 – DHHS response from Legal Services, needs clarification, “As you are aware, NDHHS no longer is involved in the program to the extent it was in the past. NDEE now manages the program and its activities. We have reached out to the NDHHS
program personnel, but the responsible employees were transferred to NDEE in July of 2021.”
November 29, 2023 Revised records request and 2/13/24 responses below
January 12, 2024 – Records request for “a copy of the procedure and the metric used for reporting the fluoride concentration level to the CDC, whether it is a DHHS or an NDEE procedure or a combined effort and the November and December [2023] fluoride treatment reports and the monthly fluoride sample reports for July 2023 through the most current available.”
January 24 – Feb 6, 2024 NDEE Response, “We checked with program staff about the second item of your records request and there is no written procedure for reporting fluoridation data to CDC.” Water sample results received 2/6/24.
2/13/24 responses to November 29, 2023 Revised records request
- NDEE staffing levels prohibit regular submittal of fluoridation data to the CDC Water Fluoridation Reporting System. The discrepancy in the reporting data “appear to be default optimal levels.”
- DHHS is the agency authorized to regulate fluoridation. Cities and villages required to fluoridate, must do so in accordance with the rules and regulations of …. (Title 179 NAC1). Determination of compliance with those rules and regulations would ultimately be the responsibility of DHHS.
- As part of the training provided to water operators on water fluoridation, the current regulatory requirements, and their relationship to previous, and current CDC recommendations is explained in detail. Operators are informed that currently, Title 179 Chapter 1 requires that “The operation of the fluoridation program shall be such that the fluoride ion content of the water available to users …shall be in the range of 0.8 to 1.5 parts per million.” They are instructed that this range, as established in Title 179 Chapter 1, was based on existing CDC recommendations at the time the regulation was developed, and that CDC’s recommendations were changed in 2015, however the DHHS regulation has not yet been updated to reflect those changes. While references are made during the training to CDC’s revised recommendations, it is emphasized that those are currently only recommendations, and that the regulations still require that a fluoridated system provide water with a fluoride ion content of 0.8 to 1.5 parts per million.
- The range of 0.1 mg/L below to 0.5 mg/L above the optimum level was the previous operational range recommended by CDC. Current guidance provided in the Water Fluoridation, Principles & Practices M4 Manual, Sixth Edition, published by the American Water Works Association, identifies +/- 0.2 mg/L of the optimal level as an achievable operating range.
Public Records Provided
- NDHHS Title 179 – Chapter 1, Rules and Regulations Governing Fluoridation of Water Supplies – effective date 8/27/1983 (effective date was a response to request for a dated regulation)
- Lincoln Water System Fluoride Treatment Reports 2021-07 to 2023-06
- Lincoln Water System Sample Results 2021-07 to 2023-06
- Lincoln Water System Sample Results 2023-01-01 to 2024-01-05
- NDEE October 25, 2023 Training – Dental Health Benefits, Fluoride Safety, Fluoride Testing
- LWS Fluoride treatment reports for 2023-07 to 2024-01 at this public portal – per NDEE – LWS Monthly DEQ are available for Lincoln Nebraska DWP 999333, NE3110926. Under DEQ Facility Number, insert 999333 Under DEQ Program ID, insert NE3110926 Click on Search
Lincoln Water System (LWS) Quality Report 2022 (link to current report) requested , copy of 2022 Report at Archive.org